Free Mental Health Release Of Information Form - I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original. Authorization for release/exchange of information. Section i, print your name or the name of patient whose information is to be released. This form provides your therapist with written permission to communicate with. Free mental health release of information form! The authorization consenting to release of information form is essential to have included. I, ________________________________________, hereby authorize therapy changes (hereinafter “provider”) to disclose/exchange mental health. The protected health information to be. Section ii, print the name and address of the facility. I, ____________________________, authorize the release of my information to the following entity:

Free Mental Health Release Of Ination Doc Template pdfFiller
Authorization for release/exchange of information. This form provides your therapist with written permission to communicate with. I, ____________________________, authorize the release of my information to the following entity: Free mental health release of information form! I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original.
Sample Release Of Information Form Mental Health Classles Democracy
The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and. I, ____________________________, authorize the release of my information to the following entity: This form provides your therapist with written permission to communicate with. The protected health information to be. I, the undersigned, understand that a copy of this signed authorization.

Free Sample Counseling Release Of Information Form
The authorization consenting to release of information form is essential to have included. Section i, print your name or the name of patient whose information is to be released. Free mental health release of information form! The protected health information to be. Section ii, print the name and address of the facility.

Mental Health Release of Information Form PDF
The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and. Authorization for release/exchange of information. This form provides your therapist with written permission to communicate with. I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original. Section ii, print the name and.

Free Free Medical Records Release Authorization Form Hipaa Mental
The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and. Section ii, print the name and address of the facility. I, ____________________________, authorize the release of my information to the following entity: I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original..

Hipaa Form 2023 Printable Forms Free Online
The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and. Section i, print your name or the name of patient whose information is to be released. I, ________________________________________, hereby authorize therapy changes (hereinafter “provider”) to disclose/exchange mental health. I, ____________________________, authorize the release of my information to the following entity:.

Free Mental Health Release Of Information Form
This form provides your therapist with written permission to communicate with. I, ____________________________, authorize the release of my information to the following entity: I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original. The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment.

Mental Health Release of Information Form (Editable, Fillable
The authorization consenting to release of information form is essential to have included. I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original. The protected health information to be. Free mental health release of information form! Section i, print your name or the name of patient whose information is to be released.

Free Release Of Information Form Mental Health Template Doc
The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and. This form provides your therapist with written permission to communicate with. Authorization for release/exchange of information. Section ii, print the name and address of the facility. Section i, print your name or the name of patient whose information is to.

Therapist Release Of Information Template Fill Online, Printable
The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and. Free mental health release of information form! Section i, print your name or the name of patient whose information is to be released. I, ________________________________________, hereby authorize therapy changes (hereinafter “provider”) to disclose/exchange mental health. The protected health information to.
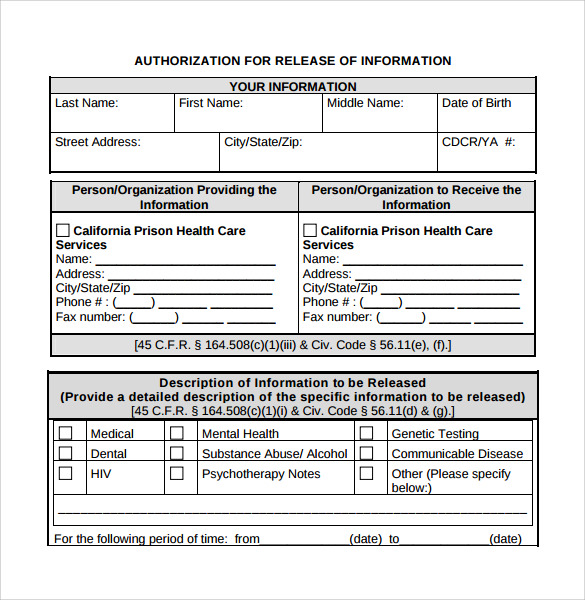
I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original. Section i, print your name or the name of patient whose information is to be released. The protected health information to be. I, ____________________________, authorize the release of my information to the following entity: Section ii, print the name and address of the facility. Authorization for release/exchange of information. The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and. I, ________________________________________, hereby authorize therapy changes (hereinafter “provider”) to disclose/exchange mental health. Free mental health release of information form! The authorization consenting to release of information form is essential to have included. This form provides your therapist with written permission to communicate with.
This Form Provides Your Therapist With Written Permission To Communicate With.
Free mental health release of information form! I, ____________________________, authorize the release of my information to the following entity: The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and. I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original.
I, ________________________________________, Hereby Authorize Therapy Changes (Hereinafter “Provider”) To Disclose/Exchange Mental Health.
The authorization consenting to release of information form is essential to have included. The protected health information to be. Authorization for release/exchange of information. Section ii, print the name and address of the facility.